September 5, 2018
Hope for food allergy sufferers
Two CBC affiliates, Cathy Nagler and Jeff Hubbell, UChicago, explain recent research progress on preventing food allergies
In the September 2018 issue of the Chicago magazine, the author Lauren Williamson intertwines personal anecdotes with a progress report on the current state of food allergies’ prevalence and available treatments. Two UChicago scientists, Cathy Nagler and Jeff Hubbell, are described as a ‘dream team’ that may contribute to the long-awaited end to this growing health problem. Both, Nagler and Hubbell are affiliated with the CBC. Previous work in the Nagler lab was supported in part by the CCSB/CBC Fellowship, awarded to a postdoctoral fellow in her lab, Aly Azeem Khan. The fellowship was financed by the CBC Lever Award (2008) for the project “Chicago Center for Systems Biology (CCSB).” Jeff Hubbell is a CBC HTS Award (2016) recipient. Congratulations!
The number of people with food allergies has exploded in recent years. A dream team of Chicago researchers and scientists may have figured out why, and now they’re developing therapies that could lead to …
…The End of an Epidemic
Chicago magazine | by Lauren Williamson | September 2018 issue

The most common food allergies. Photo credit: Clint Blowers.
The boy in the plastic bubble has nothing on the mice in Cathy Nagler’s immunology lab at the University of Chicago. They spend the entirety of their lives in impervious Plexiglas cages. The only way to access them is by reaching in with arm-length gloves that hang inside out from the sides of their cages, like a collection of spare limbs discarded by the Stay Puft Marshmallow Man. Like many mammals, mice are born with a sterile gut that’s populated over time with trillions of commensal bacteria — the so-called good flora that a healthy immune system depends on. But starting at 2 weeks old, Nagler’s mice receive antibiotics to prevent any microbes from colonizing.
Their blank-slate guts could make them the unsung heroes of a revolution in the way we prevent and treat food allergies. Back in 2004, Nagler, then a professor at Harvard Medical School, was one of the first researchers to suggest that intestinal bacteria help regulate the immune system. When she gave peanut protein to germ-free mice, they became allergic to it. Some simply got a little itchy behind their ears; others went into full-blown anaphylactic shock and died. Ever since, her work has focused on figuring out how exactly the microbiome — essentially, our body’s internal ecosystem of natural microbes — protects us against food allergies and how we can fix one that’s broken.
A treatment for food allergies has eluded researchers for the 100-plus years that the diseases have been recognized. Right now, the standard of care is still shockingly rudimentary: Don’t eat the trigger food. If you accidentally do and suspect anaphylaxis — signaled either by two or more initially mild symptoms like nausea and a runny nose or by a single big one like a puffed-up tongue — inject epinephrine, hope your airways don’t close up, and call 911. Good luck.
That’s a tremendous burden to live with, knowing that if you are allergic to, say, eggs, you could die if a speck of one gets on a hamburger because it was cooked on the same griddle as breakfast. My 20-month-old son, William, was diagnosed with a food allergy as an infant after a pebbly red rash spread across his chin the first and only time he licked peanut butter from my fingertip. When he tried eggs, whipped into a chocolate cream pie, a trio of hives rose above his upper lip. A visit to the allergist confirmed, through blood and skin tests, what we suspected — and added almonds as another likely allergen, though we won’t know for sure until he eats one. (Existing tests are maddeningly imprecise: They only measure the probability of an allergy and must be triangulated with reaction history or a food challenge that entails eating the food under a doctor’s supervision.) For now, we have to function as if William can’t eat three of the socalled top eight allergens. In addition to eggs, peanuts, and tree nuts, the other top allergens are milk, wheat, soy, shellfish, and fish.
I asked the doctors if my 1-year-old’s food allergies will be a lifelong burden. Their answer: Not even by the time he’s in junior high.
Diagnosis comes with a persistent low-grade anxiety that spikes slightly with every meal and snack. More than 40 percent of children with a food allergy have a severe reaction at some point, according to a landmark study conducted by Ann & Robert H. Lurie Children’s Hospital of Chicago. (The number jumps to nearly 60 percent when you include adults.) In the most severe reactions, blood pressure drops, lips turn blue, and the body goes limp. In any given year, one in five kids with a food allergy ends up in the emergency room. Anaphylaxis is “like watching your child drowning,” says Shannon Stevens, a stay-at-home mother in Roscoe Village whose 9-year-old son has seven food allergies.
So far, we’ve been able to avoid that terror. Most of the time, William’s allergies are just a bummer. When we go out to eat, we have to wipe down the table and highchair before strapping him in. We’ve called food manufacturers to figure out our go-to bread, chicken broth, and pasta. There’s a six-pack of egg-free cupcakes I baked waiting in the freezer at his daycare so he can get a treat on party days like everyone else. These are all minor inconveniences. But they chip away at feelings of normalcy in a culture that relies so much on food for bonding and reward.
$4,184
Annual cost to manage one child’s food allergy
The more I learned about the latest research into the prevention and treatment of food allergies, however, the more hopeful I became that it might not always have to be this way. Medicine and science are on the cusp of stunning breakthroughs — and we have a dream team of brainpower right in our own backyard. Chicago is home to experts at the forefront of almost every area: epidemiologists crunching numbers to help us understand prevalence and severity, doctors conducting clinical trials for the first Food and Drug Administrat ion–approved food allergy drugs, and scientists like Nagler and her partners at the University of Chicago who seek to alter food-allergic bodies from deep within the digestive tract.
I posed the same question to each researcher I spoke with: Will food allergies be a lifelong burden for William? Every person gave me the same answer: They will be a lifelong illness, certainly — the science is still far from a wholesale cure — but they will not be a lifelong burden. Not even by the time he enters junior high.
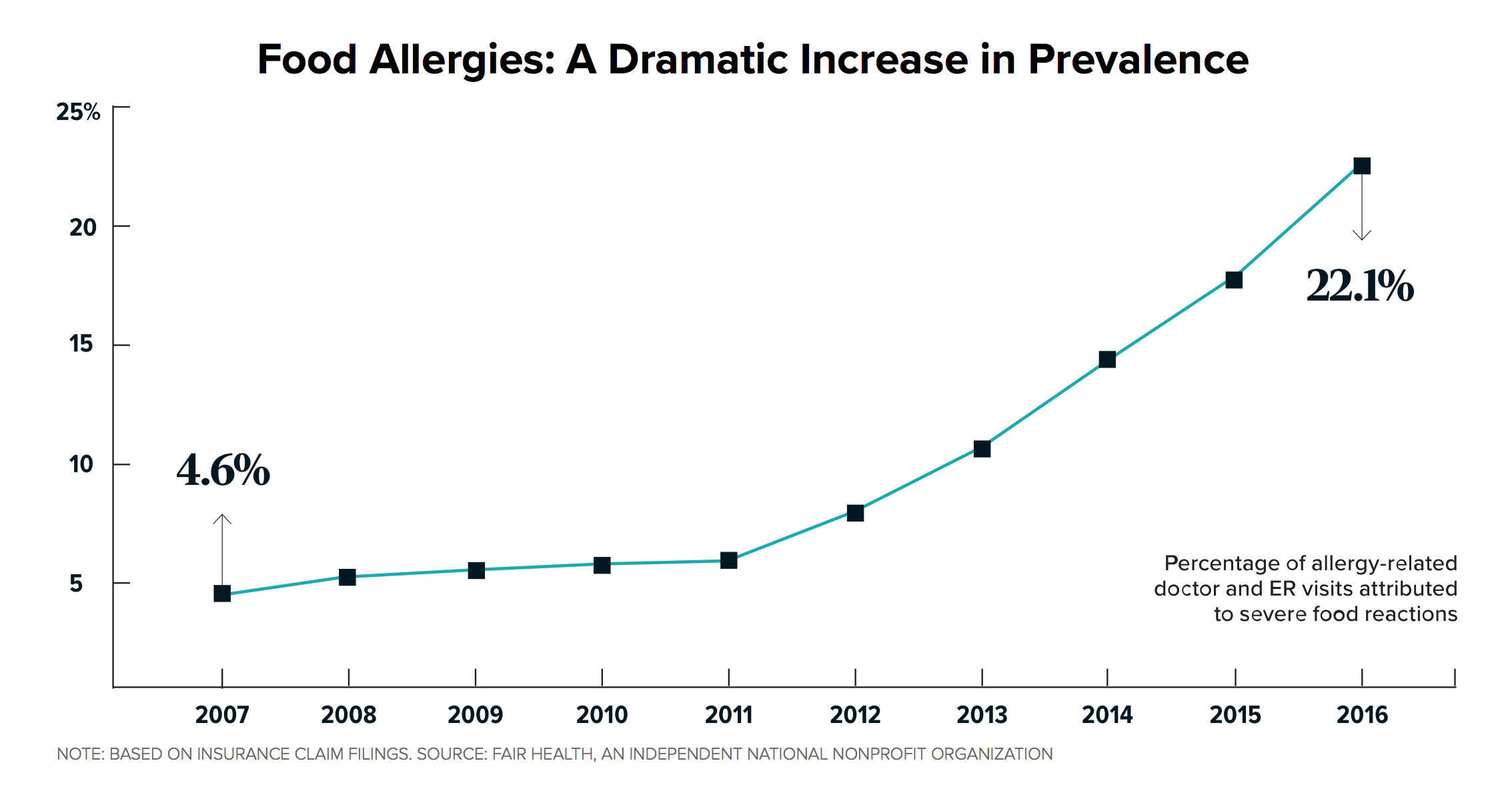
NOTE: BASED ON INSURANCE CLAIM FILINGS. SOURCE: FAIR HEALTH, AN INDEPENDENT NATIONAL NONPROFIT ORGANIZATION.
All parents of school-age children know about the peanut-free lunch table and the list of approved snacks for classroom celebrations — neither of which was a thing when they were kids. Indeed, the epidemic of food allergies has been very recent, one that first became apparent in the mid-’80s. Between 2007 and 2016 alone, the number of reported anaphylactic reactions increased nearly 400 percent in the United States, according to James Baker, who retired in June as CEO of the advocacy organization Food Allergy Research & Education, which has an office in Skokie.
And yet so much is still unknown. “If you had told me in 1981 that AIDS would be a totally treatable disease, with hundreds of drugs, and we’d have nothing to offer kids with food allergies but an EpiPen, I wouldn’t have believed you,” Baker says.
Science & Outcomes of Allergy & Asthma Research (SOAAR), the laboratory of Lurie pediatrician Ruchi Gupta, is collecting data that answer some of the fundamental questions and provide a benchmark for future research. Gupta is also a food allergy mom. Her daughter outgrew a sensitivity to egg at age 3 but is still allergic to peanuts and tree nuts. “When I go to the grocery store, I can’t buy the majority of food items, because they say ‘may contain,’ ” says Gupta, who appeared in “The Peanut Problem,” an episode of Rotten, the recent Netflix documentary about our food system. “I see the barriers to living fully. My goal is to do whatever research we can to understand how to make [life with food allergies] better.” She helped develop the American Academy of Pediatrics’ new guidelines encouraging early introduction, which were rolled out last year.
25%
Percentage of first-time anaphylactic reactions that happen at school
Research showed that kids, especially ones at high risk because of other conditions, were 80 percent less likely to become allergic to peanuts if they ate them early — between the ages of 4 and 11 months — and often. Previous warnings discouraged parents from feeding their kids peanut products before age 3. The new guidelines signaled a huge shift in the way we think about food allergies — specifically, that they might, in some cases, actually be preventable.
Roughly 8 percent of children — or two in every average-sized classroom — and 13 percent of adults have at least one food allergy, according to Gupta’s research. The discrepancy between kids and adults is revealing: Though many people think of food allergies as an issue for the very young, almost 50 percent of patients are diagnosed after turning 18. And just as with the rising rates in children, it didn’t used to be this way. Kids also used to outgrow many food allergies by age 4 or 5, but that’s not happening as often anymore, Gupta says. In particular, milk allergies — the most common type in toddlers and the third most common in adults — are becoming more stubborn.
One of the prevailing theories for the explosion is the hygiene hypothesis, says Christina Ciaccio, Nagler’s research partner and the interim head of the allergy and immunology department at the University of Chicago Medicine Comer Children’s Hospital. We have essentially given our children allergies by being too good at keeping them safe.
There’s been a huge shift in the way we think about food allergies: In some cases, they might actually be preventable.
The introduction of antibiotics and vaccines slashed infectious disease rates and should obviously be considered nothing less than a sweeping public health success story. But, the hygiene hypothesis holds, the immune system doesn’t get challenged the way it used to. Plus, antibiotics wipe out good bugs along with the bad. (It should be made very clear that no one in the medical establishment is suggesting we stop vaccinating or prescribing necessary antibiotics.) Similarly, cesarean sections have saved millions of lives, but there’s an unintended consequence. “The birth canal is strategically placed,” Ciaccio says, “so when babies are born vaginally, they essentially get a mouthful of poop, which sounds disgusting, but it’s the natural way to colonize with the right bacteria.”
Then there are the changes in our everyday life. Everything from tablecloths to shoe insoles have been infused by manufacturers with the antibacterial agent triclosan. Kids don’t play in the dirt as much, opting for video games over mud pies. We eat less fermented food, like sauerkraut and pickles. The commercially available yogurt and kefir we eat in the United States don’t do a lot for gut health, either, because they’re made with pasteurized milk. And we nourish our microbiomes poorly. They thrive on high-fiber foods, like whole grains and fresh fruits and veggies, not white bread and soda, which contain simple sugars that feed the bad bacteria rather than the good. The rise in food allergies mirrors that of other modern diseases — namely, type 2 diabetes, obesity, autism, inflammatory bowel syndrome, and asthma, which have all been linked by researchers to a depleted microbiome.
“It’s microshift, microshift, microshift, microshift,” Ciaccio says. “And just at 2018 are we finally at this place where all the microshifts over generations have landed us in this vulnerable state.”
My son’s history is a case in point. I was born by C-section, so I didn’t get my mom’s microbiome. I was almost constantly on antibiotics for ear infections and strep throat as a toddler and for chronic sinusitis in high school and college. (Incidentally, I developed several drug allergies.) William was not born by C-section, but the microbiome I gave him was lousy. Then, before he was 5 months old, it was decimated when he took two rounds of antibiotics, including a course of IV-administered clindamycin, which is brutal on good bacteria. Now that he is over a year old, his gut is what it is; Nagler says the kind of probiotics sold in stores might make him feel better if he has some stomach distress, but they won’t recolonize what’s been lost.
That doesn’t mean his immune system can’t be retrained, however, which is exactly what many of the treatments under development aim to do, either from the inside out (that is, via the gut) or, in the case of a handful of promising new approaches, from the outside in.
It’s hard to persuade drug companies to develop and test a treatment that, in some cases, involves giving children the very thing that could kill them, which is part of the reason that, until recently, the search for a cure for food allergies has been so sluggish. The research that began to be ramped up in the 2000s has finally led to what will likely be the first two FDA-approved food allergy drugs, both expected to hit the market next year.
Those two nearest-term possibilities — one a pill, the other a patch — use immunotherapy to build tolerance by incrementally increasing exposure to the trigger food. It isn’t a new concept. In 1906, a doctor in London first experimented with oral immunotherapy, or OIT, by giving a 13-year-old boy capsules containing a ten-thousandth of an egg, essentially curing his allergy after eight months of steadily increasing doses. Standardization of the technique, however, is fairly new. Research was virtually nonexistent until the mid-1980s, and it abruptly halted in the ’90s when a person died during testing of a peanut shot.
UChicago’s Cathy Nagler wants to help the gut’s natural flora retrain the immune system from the inside out.
In that fallow period, doctors continued to practice OIT, feeding patients gradually larger doses of an allergen over a period of months or years. They also turned to a variation of OIT, known as sublingual immunotherapy, in which a pat ient is prescribed drops containing minute amounts of the allergenic food to dribble under the tongue. Though these are entirely legitimate treatments, the lack of FDA approval makes pursuing them challenging. There are currently half a dozen or so generally accepted OIT protocols, including ones developed by Stanford and Duke Universities, but there’s no universal standard (which some would argue is a good thing, since allergic responses aren’t uniform, either). Insurance companies rarely cover oral and sublingual immunotherapies, and then there’s the difficulty of finding physicians who administer them — most allergists, even progressive ones, don’t.
If the two aforementioned food allergy drugs — the AR101 pill by the California-based company Aimmune and the Viaskin patch from the French company DBV — are approved, they will bring immunotherapy for food allergies into the mainstream. Jacqueline Pongracic, head of allergy and immunology at Lurie, served as a principal investigator on clinical trials for the drugs. “It took us a long time to get to this point,” she says. “But once we did, I feel like these companies have been extremely thoughtful and efficient and highly motivated to move these products forward.” While both target peanut allergies, that’s just a starting point; the science behind them could apply to any food allergy, and in fact, clinical trials are underway for a milk patch, and an egg one is in development.
Until now, peanut products from the grocery store have been used in OIT, which means there’s some natural variation in the amount of protein in each dose. AR101 and Viaskin both contain a uniform concentration of peanut-derived protein, so doctors can control exactly how much the patient gets, Pongracic says. The quantity in the AR101 pill increases every two weeks, starting with the equivalent of a five-hundredth of a peanut; people take it by sprinkling the contents of the capsule on applesauce or another food. The Viaskin patch is applied for gradually longer intervals and eventually worn 24 hours a day, seven days a week.
After one year on AR101, 67 percent of children were able to tolerate the equivalent of two and a half peanuts, according to phase 3 clinical trial data released in May. Preliminary results seem similar for adults.
Two peanuts doesn’t sound like a lot. But to people living with food allergies, that’s life changing — a threshold many refer to as “bite-proof.” Pongracic puts it this way: “If their goal is to stop carrying an epinephrine auto-injector, that’s really not going to happen with these treatments. But if their goal is to know they’re not going to have a bad reaction from a cross-contamination exposure, I think that’s something that these products can help them with.” In other words, you won’t be able to eat a whole PB&J, but nothing catastrophic will happen if you accidentally chomp into the wrong sandwich.
Those results make it sound like a miracle drug, but it’s not quite that simple. Any OIT regimen is a major undertaking. Patients must commit to a two-hour rest period after dosing because raising the body temperature can trigger anaphylaxis, Pongracic says. It’s OK to engage in normal activities, like office work or quiet play, but anything athletic is a no-go. Hormone changes during puberty can also disrupt the process. Some patients in the AR101 trial did have reactions, which ranged from an upset stomach and a sprinkling of hives to, in one case, anaphylaxis. Typically, anyone who pursues immunotherapy must first do a food challenge to confirm the allergy and set a benchmark for how much of the allergen they tolerate — which also essentially means inducing anaphylaxis on purpose.
Viaskin’s outcomes have been less clear. In the phase 3 trial last fall, a little more than a third of kids ages 4 to 11 could eat about three peanuts after a year, and stock in DBV plunged on the news that the trial failed to show a difference between the drug and a placebo big enough to meet a target set by the FDA. However, another study of Viaskin showed that one year might not be a fair time frame for assessing its effectiveness. When kids wore it for three years, not only did more respond — 83 percent — but they were also able to tolerate nearly twice as many peanuts. Only about 2 percent of kids in the trial had to drop out because of side effects, the most common of which was skin irritation. And unlike the pill, the patch doesn’t require a rest period.
Both companies plan to apply for FDA approval by the end of the year. It’s not clear yet how much the treatments will cost or what percentage of that cost insurance companies will cover. For now, immunotherapy continues to require a lifetime of daily dosages followed by a rest period, so pursuing it is a profound decision to make on behalf of a child. It’s still not known what long-term maintenance would involve for people on AR101 or Viaskin, Pongracic says, though most likely they’d eventually be able to eat, say, a couple of peanut M&Ms each day to maintain therapeutic exposure to the trigger food, rather than having to take the medications for life.
The 9-year-old in Roscoe Village with multiple food allergies is in the midst of the Viaskin trial for the milk patch. Stevens doesn’t know yet how well it’s working for her son because doctors share only limited information during the trial. Occasionally, the boy gets rashes on his back, but he’s suffered no other ill effects. Even in the absence of concrete answers, wearing the patch has given him a clearer understanding of his allergy. “It’s helped him emotionally around some of the anxiety,” she says. “I can say, ‘You have milk on your back right now. You’re not going into anaphylaxis.’ ”
Originally, her son had 12 food allergies but outgrew five on his own. Somehow, his body flipped a switch and learned not to attack what nourishes it. Immunotherapy is one way to coax that process along, but researchers believe it’s not the only way. Indeed, scientists across the country are developing food allergy vaccines and conducting trials that pair existing anti-infålammatory drugs such as Xolair with immunotherapy. (One such trial is in progress at Lurie right now.)
On their own, these treatments show great promise, but they have the potential to be even more effective if we also repair our busted guts.

Prof. Cathryn Nagler
Which brings us back to Cathy Nagler’s germ-free mice. Stripped of all bacteria that foster a well-functioning colon, they’re the ultimate test of the hygiene hypothesis. In a follow-up to her peanut study, Nagler populated their intestines with bacteria from dairy-allergic human babies. The mice started reacting to milk too. The study made it clear that a specific mixture of bacteria — or rather an absence thereof — contributes to the problem. Because something remarkable happened when healthy and allergic mice were housed together. All mice eat each other’s droppings, and in this case, the allergic ones could tolerate cow’s milk after ingesting the healthy animals’ waste. “That’s proof of the concept that it’s possible to transfer something from the [microbiome] of healthy infants to cow’s-milk–allergic infants and protect the kids,” Nagler says.
Mercifully, that doesn’t mean feeding kids poop. Having conducted additional studies, Nagler believes the key bug — the one we both starve when we don’t eat enough fiber and annihilate with antibiotic overuse — is clostridia. Its byproducts are short-chain fatty acids that regulate a protective layer of mucus in the intestines. In the absence of clostridia, this layer breaks down and allows proteins to pass into the bloodstream, where, in some people’s bodies, they are mistaken for invaders and attacked: That, in essence, is the moment an allergy begins.
Although most proteins break down in the stomach, peanut and milk proteins don’t, which is why, Nagler theorizes, they’re among the top eight allergens. (Similarly, some research points to broken skin, like that caused by eczema, as another risk factor since it allows food to enter the body in a way it’s not supposed to, causing the immune system to respond by going full spider monkey on the protein.)
Clostridia itself is fragile and quickly dies when removed from the bowel and exposed to oxygen. The shortchain fatty acids it creates, however, do not, and they can likely be re-created in a lab. Nagler and Jeffrey Hubbell, a molecular engineering professor at the University of Chicago, founded the company ClostraBio in 2016 to do just that: identify the key byproduct and turn it into a pill.

Prof. Jeffrey Hubbell
Over the past two years, they’ve received around $3.5 milion in seed money, including an infusion last winter from Joe Mansueto, the billionaire founder of the investment firm Morningstar. The majority of the benefactors up to that point had been what Nagler refers to as “love donors” — people contributing in the hope that ClostraBio will help their families. “Mansueto has no relationship to food allergies,” she says. “When he became an investor, then it kind of changed the picture because here’s sobody who’s intere-sted in this company as a way to make money.”
Nagler and Hubbell have identified a short-chain fatty acid called butyrate as a starting point. It’s one of the three most common that gut bacteria produce after they metabolize fiber. It’s been used in synthetic form to treat patients with sickle cell anemia for 50-some years, with minimal side effects. Right now, however, it breaks down too quickly if it’s not delivered intravenously, making it impractical for a drug that must be taken daily, in many cases by children. So, additionally, they must figure out a polymer that will keep butyrate from disintegrating long enough to make it into the large intestine.
Nagler doesn’t want to speculate at this point on how far out ClostraBio is from its first clinical trial with butyrate. In the nearer term, Nagler is coming at commensal bacteria, including clostridia, from the other direction, too, by researching a treatment that provides them with the fuel needed to produce short-chain fatty acids on their own and boost that protective layer of mucus. That fuel is called a prebiotic, which is a fancy way of saying fiber. Ciaccio, who is an adviser to ClostraBio, expects to begin leading the first clinical trials of a prebiotic therapy next year.
Nagler envisions these treatments as supportive therapies that, in many cases, would be taken alongside an immunotherapy regimen so that as patients retrain their immune system, they’re also restoring the gut to its proper role in immune function. In some kids, the therapies on their own might be enough to persuade the immune system to shift and start erasing the allergy. Finally, they could also be given preventively to infants at high risk of developing food allergies — ones who were born by C-section, for example, or who received several courses of antibiotics at an early age, as William did. Long-term dosage isn’t yet known. Patients might have to take ClostraBio’s drug for the rest of their lives, but maybe not. “We hope that it would cause a positive feedback loop,” Nagler says. The presence of more short-chain fatty acids might foster conditions where commensal bacteria thrive, eventually making the therapy self-sustaining.
Given that it will be a while before these treatments enter clinical trials, let alone become commercially available, and that Viaskin and AR101 will most likely be approved only for children older than 4 or 6 because doctors want to give younger children time to outgrow their allergies — the holy grail of outcomes — I wanted to know what I can do now to make it more likely William will do just that. Really, it comes down to a fundamental piece of medical advice that is simple and cheap to follow: Feed your kid fiber. Nurture the good bacteria that’s left — it may be beaten down, but it’s there.
So every day, my husband and I fill William’s tray with avocado and black beans, fresh berries and spaghetti squash. He gleefully smashes cauliflower rice and oatmeal into his mouth by the fistful. Eating, to him, is utter joy, a fact I constantly remind myself of as I fret about his restrictions and what they’ll mean for the future. There are, after all, only three foods that might harm him — and a vast world of possibilities that could help heal him.
Source:
Adapted (with modifications) from the September 2018 issue of Chicago magazine, by Lauren Williamson.
Featured scientist(s) with ties to cbc:
Cathryn Nagler, UChicago
CBC Lever Award (2008):
▸ Chicago Center for Systems Biology
CCSB/CBC Fellowship, awarded to Aly Azeem Khan—a postdoctoral fellow working with Cathryn Nagler, UChicago, was financed by this CBC Lever Award.
Jeffrey Hubbell, UChicago
CBC HTS Award (2016):
PIs: Jason Wertheim (NU) and Jeffrey Hubbell (UChicago) for the project:
▸ Restoring the Renal Extracellular Matrix Using Engineered Growth Factors
Related:
January 18, 2018
▸ ClostraBio, a startup co-founded by UChicago scientists with ties to CBC, called a “promising, emerging venture”
October 16, 2017
▸ Cathy Nagler (UChicago), CBC community member and ClostraBio company founder, featured in Crain’s Chicago Business
September 24, 2015
▸ CBC Funding Contributes to Understanding of the Gut Microbiome’s Role in Infants with Allergies to Cow’s Milk